Ahhhh. Fuck. I’ve talked before about how Mikaere’s button is in the perfect position for him to reach when his elbows are supported on the floor (so anytime he’s lying supine). He has pulled it out numerous times, and even worse – the balloon has burst and it’s fallen out. Womp.
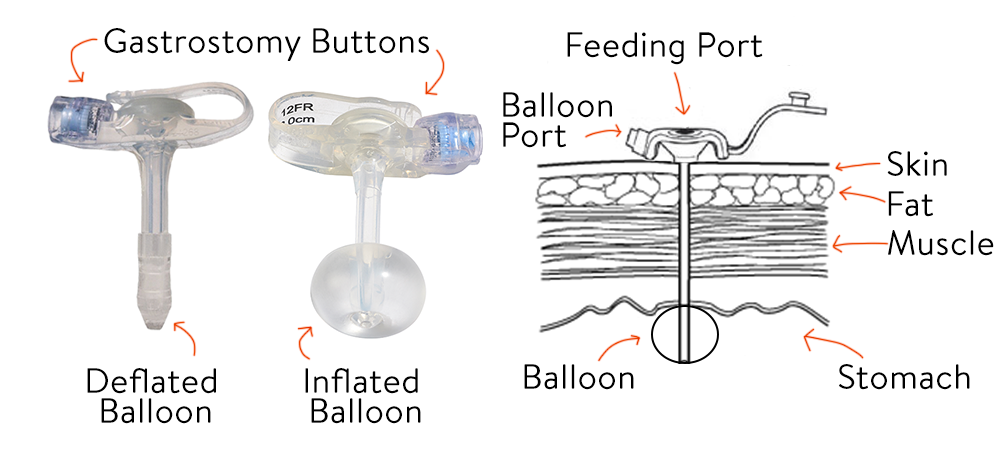
As a bit of a back history: this is what a button looks like. Essentially, there’s a feeding port with a balloon that holds it within Mikaere’s stomach. You deflate the balloon when you put it in, and once in you inflate the balloon to hold it in place. These buttons cost about £400 a pop and should last 5-6 months.
In the last 3 weeks Mikaere has had three (to the tune of £1200. W.T.F). I literally don’t understand why they’re not lasting. When I was trying to explain to our nurse what was going on, it was very confusing. In the end I had to write up a breakdown just to get my head around it:
– 14th – Button got pulled out in the carseat fully inflated. (Button A). Went into A&E for a replacement, which we put in (Button B)
– 21st – Mikaere pulled out his button fully inflated (Button B). I put Button B back in.
– 22nd – Picked up a replacement button (Button C) for just in case
– 1st – Mikaere pulled out his button (Button B) fully inflated. I put Button C in.
– 3rd – Button C had a leak and fell out. I sterilised Button B and put it in.
– 3rd – Button B also had a leak and fell out. I sterilised Button A and put it in, and taped it so it couldn’t come out.
Just in case it was hard to follow:
Button A – Currently in. Inserted twice.
Button B – leaked. Inserted 3 times.
Button C – leaked. Inserted once.
I’m getting really good at putting the button back in, but YOU GUYS – it’s always a moment of panic. It’s so terrible. First it’s because someone notices that Kai’s onsie is wet, and there’s a wet spot on his onsie right over his belly button (which is a weird place for a onsie to be wet). Whoever is nearest will jank up the onsie to check, and sure enough, the button is out and vomit is leaking out of his stoma.
It’s a bit of a race to get something – anything – into the stoma to prevent it from closing. We currently use leftover NG tubes. We have so many and they’re thin and easy to get in and tape. The concern is that if the stoma closes then 1) we’re back to the NG for meds and feeds (boo!) and 2) he’d need surgery again to put another button in. Considering the huge risk of general anaesthetic and the emotional upheaval of the first round, I’m not keen.
Once we have an ng in the stoma we can relax for a moment and figure out next steps. Sometimes that’s going into A&E if we don’t have a replacement button on hand. Sometimes it’s sterilising the existing button, letting it cool and putting that one back in. If we do have an unopened, sterile replacement we’ll usually use that.
But oh, putting it back in. It’s not as bad as the NG, but it’s not fun. Because typically Mikaere pulls out the button fully inflated, his stoma is sore and a bit tender. When I attempt to push a new one back in (deflated, obvs), Mikaere screams and clenches his abdominal muscles, essentially stopping me from pushing it through. I have to wait until he takes a breath in – when he takes a breath in his lungs expand and his abdominal muscles relax for a millisecond. Listening to your baby scream because of something you’re doing is horrid. It’s heartbreaking and I hate it. But it’s necessary, so necessary, so on we go. Eventually it’ll be in and we aspirate stomach contents up to make sure it’s in the right place (testing with a PH strip).
Having to do this 5 times in the past three weeks has definitely upped the daily stress factor of our lives. The most current button is physically taped to his body, so he’d need to get through several layers of hyperfix to the button out. We don’t have a spare at the minute, so I’m really really hoping he doesn’t pull it out. I don’t fancy a trip to A&E for another one.
We’ll see. Hopefully things will get better soon. Fingers crossed this one will stay in longer than a few days!